

Federal Crimes and Sentencing Guidelines: Health Care Fraud
Posted on by Michael Lowe.
Federal Charges for Healthcare Fraud Involving Texas Health Care Providers
Texas physicians, as well as pharmacists, clinics, and other health care providers, need to be aware of the growing risk of investigation, arrest, and prosecution for violations of federal criminal laws involving health care fraud.
Federal criminal law applying to the practice of medicine in the United States is complicated and ever-changing. (For instance, we recently discussed a change in the Federal Sentencing Guidelines dealing with punishment ranges for certain opioids (e.g., fentanyl), effective November 2018.)
Health care providers need to understand the kinds of charges they can face in a federal criminal action as well as how the United States Sentencing Guidelines apply to a healthcare fraud indictment.
Today, no one can consider themselves immune from health care fraud investigation by the federal authorities. Any provider under investigation must be vigilant in aggressively defending against federal criminal action.
Consider the following, provided by the United States Sentencing Commission in its latest Quick Facts publication for health care fraud:
- The majority of health care fraud offenders were sentenced to imprisonment (71.4%).
- The average sentence length for health care fraud offenders was 29 months.
- In fiscal year 2016, more than half of health care fraud offenders were male (54.0%).
- The average age of these offenders at sentencing was 48 years.
- The majority of health care fraud offenders had little or no prior criminal history (86.5% of these offenders were assigned to Criminal History Category I).
- 4% of health care fraud offenses involved loss amounts of $150,000 or less.

Charges for Health Care Fraud: Defined Crimes of Medical Providers
There are Texas criminal statutes that define health care fraud crimes under state law, as well as the more well-known federal legislation. Often, investigations into the activities of a doctor, a clinic, a pharmacy, an ambulance company, or a hospital will involve both Texas and federal law enforcement working in a joint effort to investigate fraudulent conduct.
Agents from a variety of federal agencies can be involved in an investigation into the activities of a Texas medical provider. They include not only the FBI (Federal Bureau of Investigation), but also the Department of Health and Human Services (HHS); the Defense Criminal Investigative Service (DCIS); and the Office of Personnel Management (among others).
Federal Health Care Fraud Statute
While a provider can face charges under Texas and/or federal law, today we focus on the federal statute found in 18 U.S.C. §1347, which defines the federal offense of healthcare fraud. The federal law is very broad, and realistically can be applied in almost every case.
The federal healthcare fraud statute makes it a federal crime for any entity to try and defraud any health care benefits program with the intent to gain control of something of value, i.e., either money or property.
The prosecution will delve into two issues:
(1) Did the provider knowingly and willfully try to defraud a healthcare benefit program by submitting claims for services or products that were never provided? or
(2) Did the provider provide services that were not medically necessary?
It will not matter that the provider has no actual knowledge of this criminal law. It does not matter if the provider lacked any specific intent to commit a violation of this statute. 18 U.S.C. §1347(b).
Other Federal Criminal Laws for Health Care Fraud
While the federal health care fraud statute is the most common violation asserted in a federal criminal prosecution against a medical provider, it is not the only option available to prosecutors with the Office of the United States’ Attorney General.
As discussed in the United States Attorneys’ Manual, medical providers can also face charges based upon:
Specific statutes here include the following: 18 USC § 669 (theft or embezzlement in connection with healthcare matter); 18 USC § 1035 (false statements relating to healthcare matters); 31 USC § 3729 (False Claims Act); and, 18 U.S.C. § 1028A (Aggravated Identity Theft /Identity Theft Penalty Enhancement Act).
The federal government will not hone their focus to a single statute or criminal act. If possible, the medical provider will be arrested on a variety of federal charges. For instance, a charge of violating the federal health care fraud statute may be tied with violations of money laundering laws and mail or wire fraud, which then allows the application of the federal forfeiture statutes.
Defending Against the Prosecution of Federal Health Care Fraud
The faster a medical provider enlists the aid of an experienced criminal defense lawyer, the better. These are complicated cases, where the doctor (or clinic, pharmacist, etc.) is arrested only after a detailed investigation has been conducted to gather sufficient evidence to support the indictment.
A criminal defense that begins after the indictment is running fast to catch up with the weeks or months of work already undertaken by the federal investigators. Voluminous documentation is likely to be involved, insofar as the invoicing, insurance claims, medical histories, and more used by the AUSA as proof in the case.
Accordingly, the criminal defense in a health care fraud case is physically complicated. It is also complex in other ways. The attorney must understand aspects of the medical practice and its administration, as well as having some knowledge about the actual medical services provided by the provider. This dovetails with the lawyer’s understanding of the applicable laws and statutes as well as their case precedent applications.
Aggressive criminal defense begins at the outset, challenging not only the substance of the proof being used against the physician but the procedures that have been or that are being followed in the case.
- Is the evidence admissible?
- Has every document been authenticated?
- Are there flaws in the government’s meeting of its burden to prove any element in any of the charges?
- Were there constitutional violations made during the investigation or arrest (fruit of the poisonous tree)?
In some instances, the defense can achieve victory with the healthcare fraud case being (1) dismissed (a) before trial after an evidentiary hearing before the trial judge, or (b) in trial, after the prosecution has put on its case in the courtroom; or with (2) the jury coming back with a not-guilty verdict.
However, in other situations, the medical provider’s success will be found in the negotiation of a plea deal and the sentencing itself. In these federal health care fraud prosecutions, there is little to debate in the establishment of a violation of the federal health care fraud statutes.
Instead, the defense will look to arguments to mitigate the sentence and to convince the judge to go outside the sentencing guidelines. These plea negotiations are complicated by the federal focus in health care fraud sentencing, which leans heavily on the alleged dollar amounts charged in the claims.
Sentencing in Federal Healthcare Fraud Cases
Federal sentencing is controlled not only by the language of the particular criminal statute and its punishment provisions, but also by the United States Sentencing Guidelines, as developed and overseen by the United States Sentencing Commission.
1. United States Sentencing Guidelines
We have discussed the background of the Sentencing Commission and demonstrated how the Guidelines work earlier. For more, see:
- Federal Sentencing Guidelines: Conspiracy to Distribute Controlled Substance Cases; and
- Federal Sentencing Guidelines on Federal Child Pornography Cases.
These guidelines will tally a range of punishments to be applied by the judge as calculated using the Sentencing Manual. These guidelines are not mandatory, and the federal judge may have the power to make his or her sentencing decision outside the guideline recommendations.
Base Offense Level
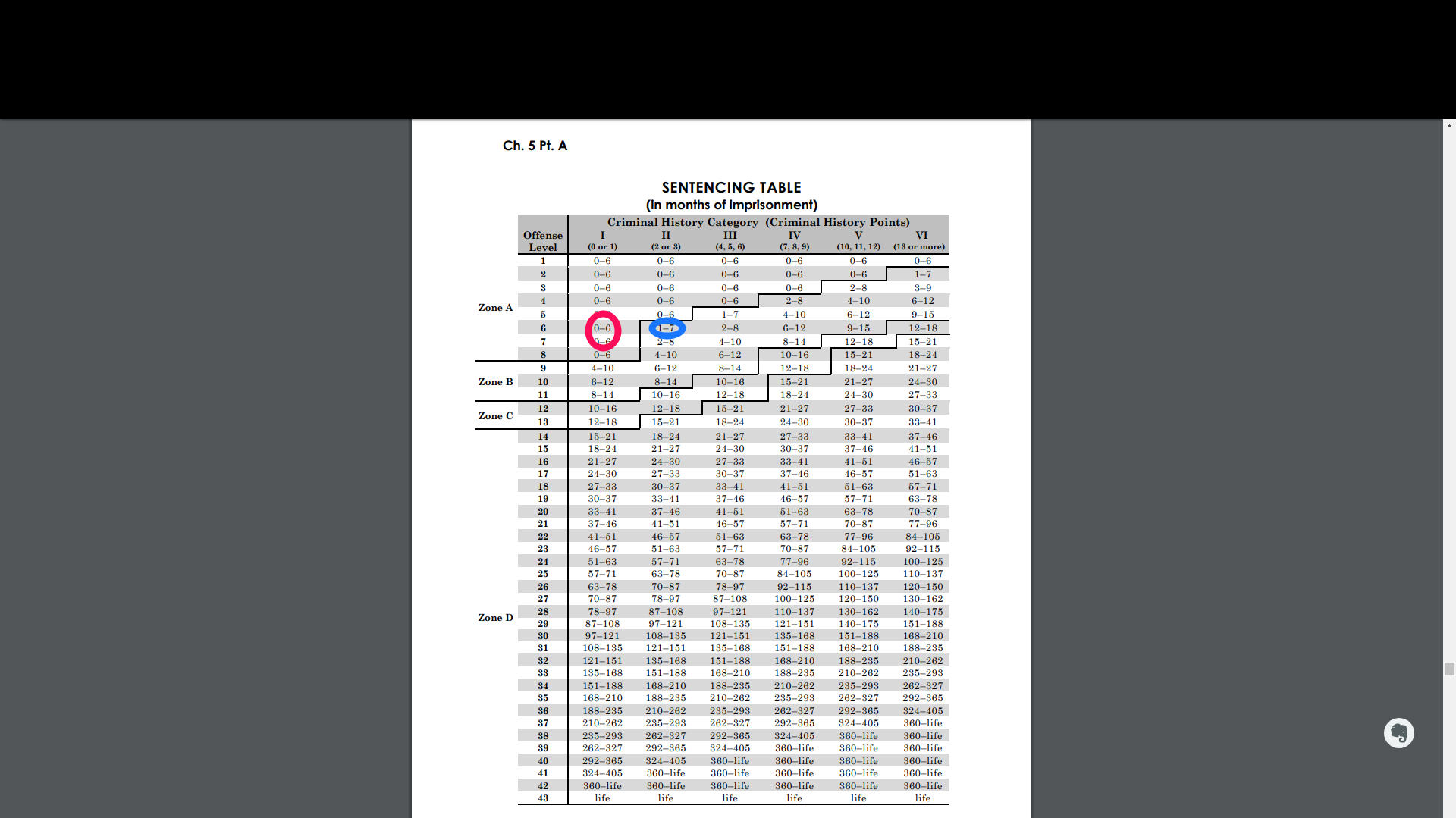
In Health Care Fraud Sentencing, the punishment calculation starts at a Base Offense Level 6 in the Sentencing Table. Assuming the doctor has no criminal record, his or her starting point will be a sentence of 0-6 months (see level 6 in the “Criminal History Category I” column). Look to Zone A, and the doctor may be given probation.
See the pink circle in the Sentencing Table example below.
Things change if the physician has a criminal record. His starting point in the Sentencing Table will be found at level 6 in the “Criminal History Category II” column. This comes with 1-7 months imprisonment as her starting point. The doctor may be given probation with confinement.
See the blue circle in the Sentencing Table example below.
Increasing or Decreasing Offense Levels
After this calculation, there will be consideration of the offense levels. The proposed sentence may increase or decrease under the Guidelines Manual, depending upon the circumstances of the case. For instance:
- If the doctor billed over $1,000,000 in government health insurance claims, then the offense level goes up (see, e.g., 2016 Sentencing Manual §2B1.1(b)(8)); but
- If the doctor accepts responsibility for her actions and shows remorse to the court for her activity, then her offense level goes down. (see, e.g., 2016 Sentencing Manual §5K1.1).
These Guideline factors are not mandatory, but courts follow them and when they do, the sentences are presumed to be reasonable. There are other statutory factors that courts may take into consideration to justify a departure from the Guideline sentencing range, in addition to other exceptions and motions that can affect the final sentence.
2. Statutory Sentencing Ranges
Insofar as healthcare fraud sentencing, there are several sentencing ranges defined in the federal statutes. Here, the law itself establishes maximum sentencing for violation. For instance:
A. Health Care Fraud (18 USC §1347)
- Ten (10) year maximum sentence
- Twenty (20) year maximum sentence if serious bodily injury to patient
- Life sentence if death of patient involved
B. Controlled Substances Act (21 USC §841)
- 1 year maximum sentence for distribution of Schedule V drugs
- 5 year maximum sentence for distribution of Schedule IV drugs
- 10 year maximum sentence for distribution of Schedule III drugs
- 20 year maximum sentence for distribution of Schedule II drugs
- 20 year maximum sentence for distribution of Schedule I drugs
C. Money Laundering Act (18 USC §1956)
- 20 year maximum sentence
The statutory sentencing ranges are different from the Sentencing Commission’s Recommendations in its Sentencing Manual. These federal laws come with specific sentencing range requirements that must be followed by the court.
For instance, if a pain management clinic owner and operator is found guilty of violating the Controlled Substances Act in the distribution of opioids, then he or she will facing sentencing under the mandatory provisions of that statute. For more here, see our earlier discussion of how the sentencing guidelines are applied in Controlled Substances Act violations.
3. Health Care Fraud Sentencing Hearing
The actual sentence for the individual will be based upon oral arguments made by both the prosecutor and the defense attorney to the federal judge. They will each file their supporting documentation (briefs, Pre-Sentencing Reports (PSRs), memoranda) prior to the hearing for the judge’s consideration, as well.
The sentencing hearing will include the presentation of evidence by both sides. The defense will be able to provide expert testimony to support its arguments that the judge should not look exclusively to the statutory sentencing ranges nor to the Sentencing Guidelines, but he or she should consider the unique and particular mitigating circumstances of the particular medical provider’s situation.
How Often Will The Judge Deviate From The Health Care Fraud Sentencing Guidelines?
Statistics show the 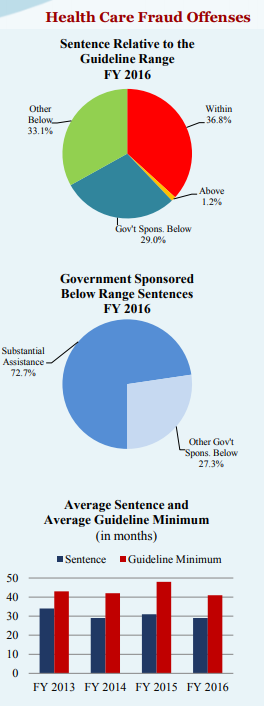 likelihood of a decreased sentence in a healthcare fraud case is increasing. Consider the following, again supplied by the United States Sentencing Commission’s latest QuickFacts:
likelihood of a decreased sentence in a healthcare fraud case is increasing. Consider the following, again supplied by the United States Sentencing Commission’s latest QuickFacts:
- Sentences for health care fraud offenders were increased for:
- Conviction of a federal health care offense involving a government health care program and a loss of more than $1 million (33.0%).
- Use of sophisticated means to execute or conceal the offense (16.4%).
- Leadership or supervisory role in the offense (19.9%).
- Abusing a public position of trust or using a special skill (28.1%).
- Obstructing or impeding the administration of justice (4.8%).
- Sentences for health care fraud offenders were decreased for:
- Minor or minimal participation in the offense (8.3%).
- Sentences relative to the guideline range:
- During the past four years, the rate of within-range sentences for health care fraud offenders has decreased from 43.6% in fiscal year 2013 to 36.8% in fiscal year 2016.
- Substantial assistance departures were granted in approximately 15 to 23 percent of health care fraud cases in each of the past four years.
- In each of the past four years, approximately 33 percent of health care fraud offenders received a non-government sponsored below range sentence.
- During the past four years, the average sentence for health care fraud offenders and the average guideline minimum for these offenders decreased overall. The average sentence imposed decreased from 34 months to 29 months during that time period. The average guideline minimum decreased from 43 months to 41 months during that time period.
Arguments in Defense of Medical Provider in Health Care Fraud Sentencing
Experienced criminal defense lawyers will have past experience in dealing with the federal prosecutors, and can use that history with the AUSA in the defense of the case, including negotiation of a plea deal or sentencing recommendation.
Dealing with the AUSA
For instance, the medical provider’s defense attorney usually will be open to a meeting with the AUSA early on in the case, if only to discuss with the prosecutor what the government considers its key documents in the large volume of evidence that usually accompanies these investigations.
This helps the defense team to assess the likelihood of a conviction and whether or not it is in the best interests of the accused to enter into plea negotiations. Determining the strength of the prosecution’s case and the viability of a successful defense is critical. With the accused’s understanding and assent, plea negotiations can begin and move forward if the likelihood of conviction is high.
The AUSA should be willing to discuss a plea deal, even if he or she is confident of victory at trial. The AUSA’s caseloads may be extensive, for one thing. Their work load alone may be incentive to negotiate.
Calculating the Sentencing Range
The defense must then consider the United States Sentencing Guidelines carefully, as well as the applicable statutory sentencing ranges imposed by the specific health care fraud laws involved in the case.
There will be several possible results to consider and compare: from the optimal result for the defendant, to what the result may be should the case goes to trial and sentencing occurs after conviction (evidence at trial may impact the guidelines).
The lawyer must not only do so in order to argue his position on the proper sentence in the case, he must do so in order to confirm any errors made by the government in its sentencing calculations.
Arguments to be made during health care fraud plea negotiations can include arguments like:
1. What is The Actual Loss Amount?
Pursuant to United States v. Isiwele, 635 F.3d 196, 203 (5th Cir. 2011), in a health care fraud case, the amount fraudulently billed to the federal insurance program (Medicare or Medicaid) is “prima facie evidence of the amount of loss [the defendant] intended to cause,” but there can be additional evidence presented by the defense to demonstrate that this total “exaggerates” the defendant’s intent.
Does the government’s tallied total loss amount inflate or exaggerate the accused’s real intent? If so, then the loss amount must be reduced in sentencing considerations.
2. Error in AUSA’s Guideline Projections
Before meeting with the defense, the AUSA will have undertaken his or her own sentencing guidelines analysis. Having a thorough understanding of your client’s case as well as the applicable law, another argument to be made in plea negotiations is how the sentencing guidelines apply in the situation.
The AUSA’s projections may be inaccurate. They usually do not jive with the Pre-Sentencing Report’s analysis. Miscalculations can form the basis of negotiating a lower sentence for the health care defendant.
___________________
Health care defendants often have never been investigated for any criminal wrongdoing, much less arrested and charged with an offense. Having an experience criminal defense lawyer as their advocate in dealing with federal authorities is paramount.
For more information, check out our web resources, read Michael Lowe’s Case Results, and read his in-depth article, “Relevant Conduct in the Federal Sentencing Guidelines: Acquittals And Uncharged Conduct.”
Comments are welcomed here and I will respond to you -- but please, no requests for personal legal advice here and nothing that's promoting your business or product. Comments are moderated and these will not be published.
Leave a Reply